Passage of the One Big Beautiful Bill Act (H.R. 1) in the U.S. House has sparked discussions about the impact of reductions in federal funding across the U.S. KFF, a nonprofit policy analysis organization formerly known as Kaiser Family Foundation, estimates that the House Budget Committee’s reconciliation bill would reduce federal Medicaid spending by $791 billion without accounting for interactions that would lower estimates to $723 billion. Almost 85% of the total savings derived from five features:
- Mandating work and reporting requirements ($280 billion),
- Repealing rules simplifying Medicaid eligibility and renewal ($167 billion),
- Creating a moratorium on new or increased provider taxes ($89 billion),
- Revising state-directed payment limitations ($73 billion), and
- Increasing the frequency of eligibility re-determinations for the ACA expansion group ($53 billion).
Approximately $357 billion of the reductions would only apply to states that adopted ACA expansion.
Federal cuts to states of $723 billion over 10 years would represent 11% of federal spending on Medicaid over the period. KFF estimates that the cuts range from 5% in Alabama, Wisconsin, and Wyoming to 15% in Washington, Louisiana, and Illinois.
Congressional Budget Office estimates a 10.3 million loss of Medicaid enrollment by 2034, representing 12% of projected enrollment in that year. At the state level, the largest reductions in Medicaid enrollment would be in Washington and Virginia, decreasing by 25% and 20%, respectively. In Alabama, that would be about 4% or approximately 47,000 people.
As described in a previous post, Alabama receives more than $60 billion in federal transfer payments to individuals from Social Security, unemployment benefits, educational benefits such as Pell Grants, or as payments on behalf of individuals in Medicare or Medicaid, etc.
As the Economic Innovation Group noted in its report, The Great Transfer-mation: How American Communities Became Reliant on Income from Government, the main reason federal transfers have increased is the increase in the percentage of the population over the age of 65. Other economic factors have contributed to a reliance on federal transfers, particularly in rural areas with declining economic conditions.
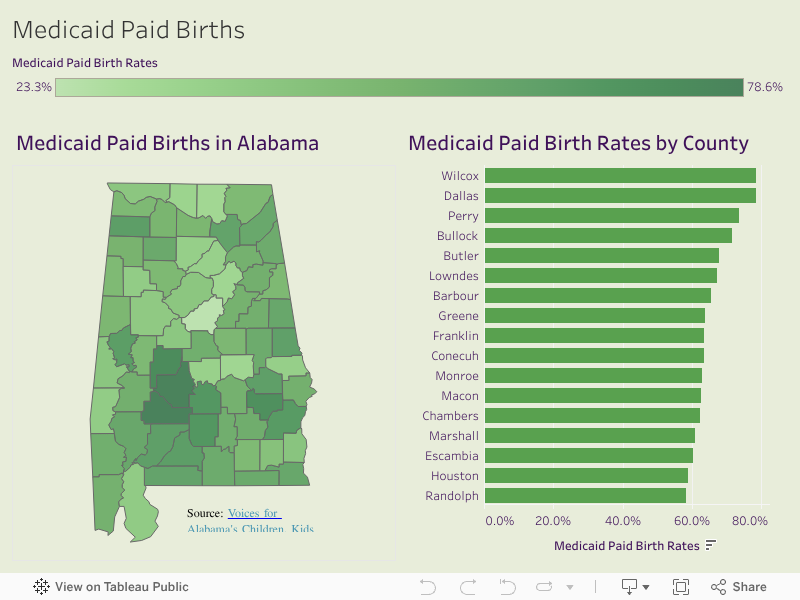
Currently, among the transfer payments are approximately $15.5 billion (2022) to medical providers on behalf of Medicare recipients and another $7.6 billion (2022) on behalf of Medicaid patients, including covering approximately 44.7% of births in Alabama in 2023. Rates vary dramatically across counties, with 78.6% of births in Wilcox County covered by Medicaid to a low of 23.3% in Shelby County. Georgetown University’s McCourt School for Public Policy found that many small towns are dependent on Medicaid/CHIP funding. With 48.6% of children in rural areas of Alabama enrolled in 2023, the state ranks 12th in the nation on that metric.
This past legislative session, the Alabama Legislature passed Senate Bill 102, expanding Medicaid benefits for pregnant women “with an estimated addition of $1 million annually for fiscal years 2026, 2027, and 2028, consisting of $726,300 in federal funds and $273,700 in state funds, by providing certain prenatal coverage to women found presumptively eligible by a qualified provider.” Governor Kay Ivey signed the bill on May 1.
Many medical facilities in Alabama depend on federal funding from Medicaid and Medicare patients. According to KFF, Medicare covered 63% of certified nursing facility residents in Alabama, while Medicaid covered approximately 13%, with only 24% covered by other private funding sources.
For the 80 hospitals in Alabama, operating margins were approximately 2.9% in 2023. However, they are generally thinner in poorer rural areas of the state. Nationwide, operating margins in rural hospitals are notoriously thin, with 44% of rural hospitals operating in the red. According to KFF, “As of July 2024, Medicaid was the primary payer for 63% of nursing facility residents; Medicare for 13% of residents; and the remaining 24% of residents had another primary payer (ex. private insurance, out-of-pocket, etc.) Medicare does not generally cover long-term care but does cover up to 100 days of skilled nursing facility care following a qualifying hospital stay.”
In states without Medicaid expansion, just over half (53%) of rural hospitals operate in the red. Reductions in Medicaid or Medicare could have a significant impact on rural hospitals. KFF reports that rural hospitals had an average operating margin of 1.7% in 2023. Reductions in these amounts, whether direct payments to individuals or payments on behalf of recipients, as in the case of Medicaid and Medicare, would reduce, dollar for dollar, the purchasing power in those communities.
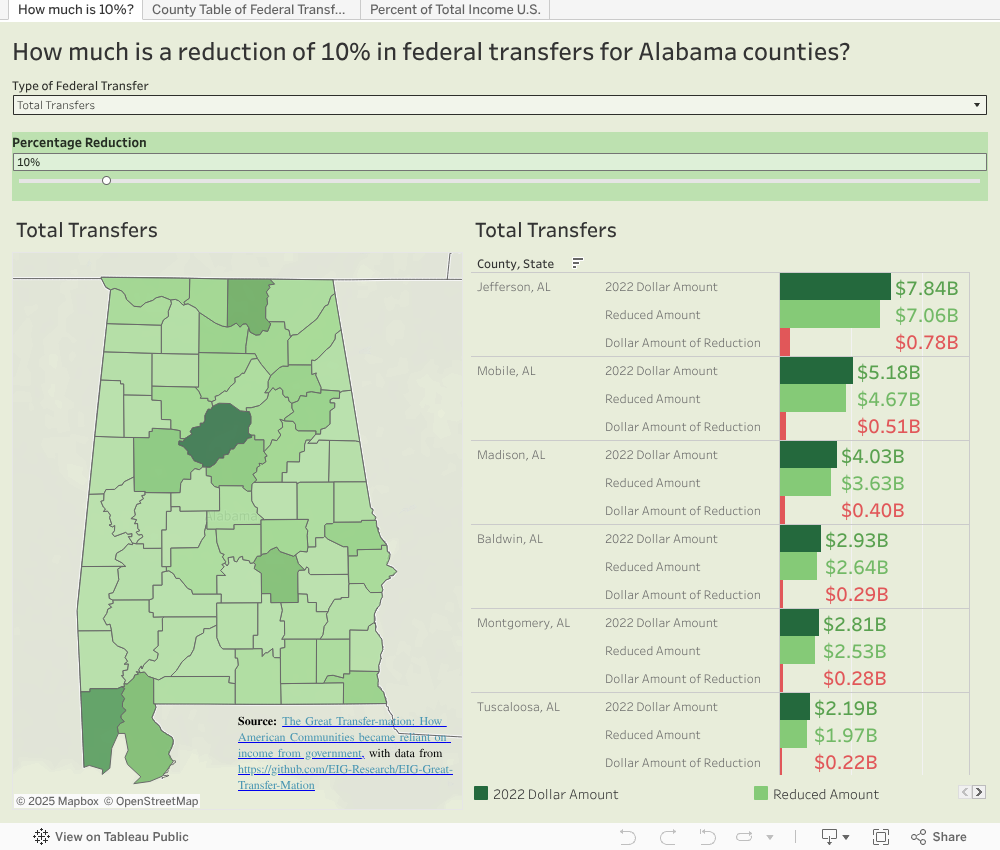
Using the slider and program selector in the visualization below, estimates of how a percentage decrease for each kind of transfer can be adjusted to find dollar amounts for hypothetical decreases:
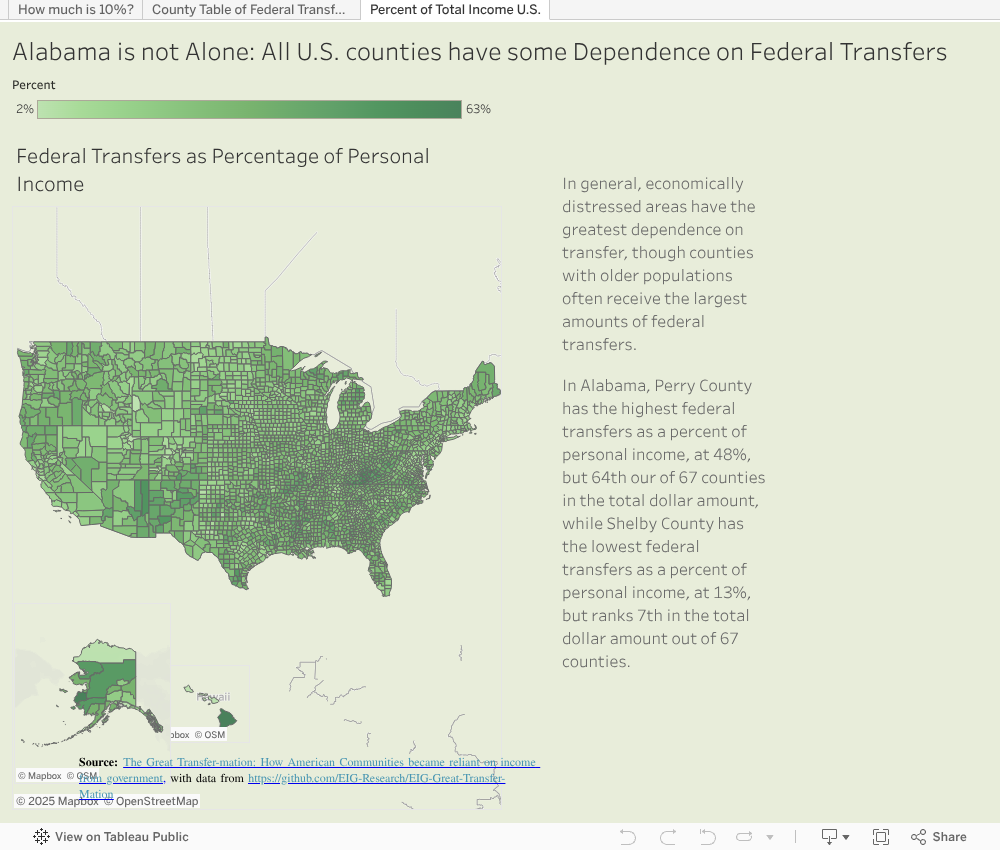
Alabama is not alone. The same kind of dependence can be seen across the country.
There are common patterns across the places where economic activity has been challenging, including the Texas Valley, the Mississippi Delta, Appalachia, and tribal territories. Still, many communities have aging populations, with high percentages of transfer payments compared to earned personal income, as shown below:
For details on the calculation of personal income and transfer payments, see this post on Github:
https://github.com/EIG-Research/EIG-Great-Transfer-Mation